PETER was a 35-year-old male with high cholesterol who had tried cholesterol-lowering tablets but had suffered aches and pains. He really didn’t want to be on medication unless it was clearly indicated. At our first meeting, he was fit and well, and was not on any regular medication. There was no history of premature coronary artery disease in his family although both his parents had had elevated cholesterol.
His levels of cholesterol are high and concerning. The absolute cardiovascular disease risk calculator estimated Peter’s risk at greater than 15 percent chance of an event in the next five years or over 30 percent in 10 years. This was a very high risk.
We spoke at some length about the role of scanning his heart to provide more information about the state of his arteries, in a bid to determine in more detail what his risk might be. I explained that he was younger than usual for such scanning. I also explained the risk of x-ray exposure and of possible contrast reactions.
Peter was keen to undergo scanning so that he could be as well informed as possible and so make the best decisions for his care. He was married with three children and he didn’t want to leave his heart health to chance. Below are the images we obtained.
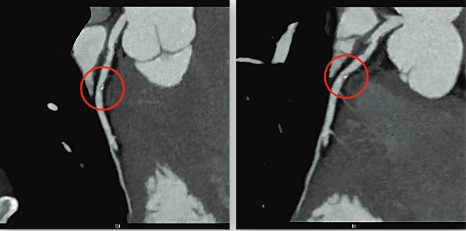
The calcium score was three and this would generally suggest a low risk of an event over the next 5 to 10 years. However, as can be seen from the images above, there is a significant amount of non-calcific plaque which carries a high risk of an event over the next 5 to 10 years if left unattended.
This information was what Peter needed to know to be clear about his health management. I indicated that he would benefit from treatment. The pictures were explicit and gone were his doubts about the benefits of taking medication.
He is now on aspirin and two cholesterol-lowering medications, and has also embraced significant lifestyle changes. The result is a major turn-around in the management of his
cardiovascular risk. He is happy with the outcome and is positive about being informed and proactive.